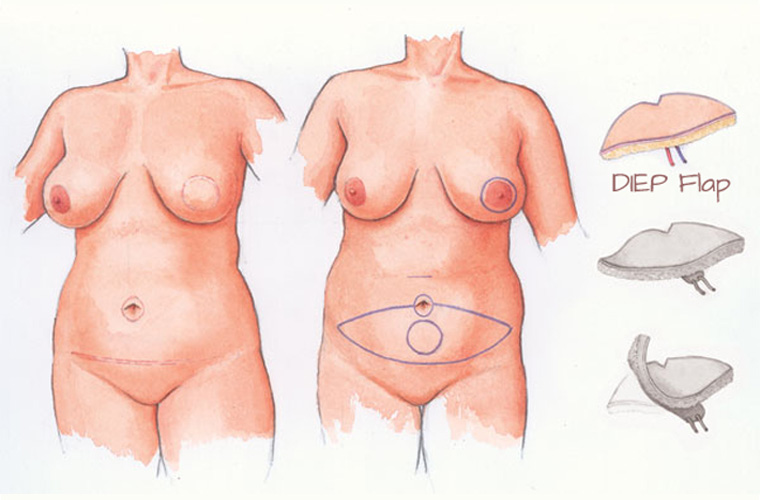
DIEP Flap
The Deep Inferior Epigastric Artery Perforator (DIEP) flap was developed from the TRAM and muscle-sparing TRAM flaps in the late 1980s.
History
The Deep Inferior Epigastric Artery Perforator (DIEP) flap was developed from the TRAM and muscle-sparing TRAM flaps in the late 1980s. Rather than take all or part of the ‘6-pack’ muscle on one side, refinements in surgical technique meant that the skin and soft tissue of the abdomen could be taken with just the required artery and veins, leaving the muscle behind. This requires precise surgical technique and is more demanding for the surgeon, but it means that the abdominal recovery and power is much better after the operation, so the chance of abdominal bulge or hernia is much less.
The Procedure
The DIEP flap is a tried and trusted reconstructive option, producing a good volume of tissue in most patients to reconstruct the breast in one sitting. Indeed, bilateral breast reconstruction can be performed. It allows surgeons to work in two teams, shortening the operating time and reducing anaesthetic complications. The scars are well hidden and tolerated and implants are very rarely required. In an immediate reconstruction with a circumareolar mastectomy, only a small disc of skin may be retained. For a delayed reconstruction much larger areas of healthy skin can be imported, than any other technique, allowing a more natural, softer breast to be reconstructed. The procedure for high risk patients having risk-reducing breast surgery where no skin is taken then the reconstruction can be buried completely.
In a minority of patients, the vessels supplying the tummy skin are two small or fragile to dissect safely, in which case conversion to a muscle-sparing TRAM may be the best option for the patient. Abdominal scars such as the laprascopic, low Caesarian or appendix scars can usually be removed with no problem. Midline scars may require the two halves of the tummy to be taken separately while a large gall-bladder incision may prevent the safe use of the DIEP flap, depending on the position and size of the scar.
Donor Site
The abdominal donor site does mimic the scar produced by a cosmetic tummy-tuck (abdominoplasty) albeit with some scarring in the muscle, as the vessels are dissected free, but the damage is much more limited than the older techniques. Additionally, not having a section of muscle underneath the flap produces a leash of vessels (pedicle) that is longer allowing more freedom in positioning the new breast, thus vessels can be utilized in the armpit (axilla) as well as behind the rib near the breast bone.
Complications
Complications can occur but our nurses and medical staff monitor the patient very closely optimising their observations and provide the best physical, and psychological, environment for wound healing. Complications can occur, requiring re-exploration, but in the majority of situations the breast reconstruction can be saved. Overall, complete loss is only 1-2% in centres that do high volumes of micro-vascular breast reconstruction.
As much as possible we aim to match the reconstructed breast to the other side, to avoid surgery on a normal breast, however, a large or droopy (ptotic) breast can be impossible to match, especially with a smaller tummy. Whenever possible symmetry surgery will be performed at the same time however, on occasions this may have to be done several months later. At the same time any scar revisions can be completed. Any radiotherapy or chemotherapy needs to be completed first and this time allows the post-operative scarring and swelling to settle. Once the breasts are more symmetrical then the final procedure is to perform a nipple reconstruction under a local anaesthetic. Followed several weeks later by tattooing of the nipple and areola complex.
SIEA Flap
In a small proportion of cases, another vessel is big enough to be used which lies just under the skin and runs parallel to the deep vessels but is more superficial. This is called the Superficial Inferior Epigastric Artery, hence SIEA flap. Advantages include a very quick dissection as the vessel is just under the skin and no dissection through the abdominal wall so no chance of a hernia or bulge. In fact the donor is identical to a cosmetic abdominoplasty so very acceptable.
Disadvantages include a much shorter length of blood vessels that can be dissected out (pedicle length) so the vessels on the chest have to be used as recipient vessels and not the ones in the armpit. Secondly, the SIEA vessel only supplies one half of the abdominal skin and does not cross the midline, so larger volumes of tissue cannot be used as in the DIEP flap, however, this is ideal for bilateral breast reconstruction where the abdominal tissue needs to be divided in two. Lastly, only a small minority of patients will have a SIEA vessel that is big enough to be used safely.
Other Procedures
Please go through the information below in your own time to help your understanding of the options available.