Delayed v Immediate
There are pros and cons to having reconstruction performed at the time of cancer surgery versus sometime later.
Mastectomy and immediate reconstruction of the breast can allow complete treatment of the breast disease (e.g. DCIS) and a new breast to be created in one sitting. We consider this the ‘gold standard’ for breast reconstruction as the native breast skin is better preserved, rather then being allowed to contract down, and the skin paddle required from the reconstruction may only be as big as the previous nipple and areola complex.
Disadvantages include another layer of options to be considered on top of cancer treatment and wound healing problems can occasionally interfere with starting chemo or radiotherapy in a small number of women. Radiotherapy can cause problems even to a well-healed reconstruction, especially if there is an implant in place. Finally, organizing a combined list for plastic and breast surgeon requires extensive resources to be in place, something that we provide for over 200 cases a year.
Other patients may prefer to deal with the cancer surgery first, as this is a significant operation on its own, plus there may decisions to be made regarding hormone, chemo and radiotherapy. The many reconstructive options can then be considered once the life saving treatment has been completed. However, the breast skin left after a mastectomy alone does tend to contract down and become adherent to the chest wall making access difficult later. Plus radiotherapy can cause excess scarring in the soft tissues and can make dissection of the blood vessels for DIEP or TRAM, extremely difficult. Lastly, those having a delayed reconstruction may have to life with an external prosthesis for a period of time and this can be problematic, especially for the larger breasted lady.
With Delayed v Immediate Reconstruction it is important to realise that there is no one best option for every lady in need of surgery as many factors come into play such as, age, occupation, medical problems, current medications, smoking, sports activities, type of cancer surgery, extent of breast disease, adjuvant therapy schedule, patient and partner’s preference. Usually, we are able to assess you and present at least two reasonable options which you can then discuss with our breast reconstruction nurses in more detail.
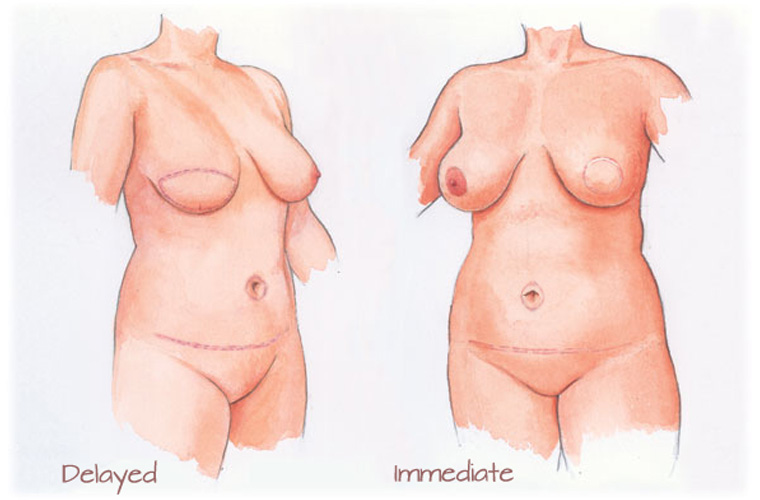
The above picture demonstrate the difference in the scars on the breast after an immediate mastectomy and breast reconstruction, when the scar will tend to end up just around the areola, compared to that of the delayed reconstruction where more skin has to be brought in and thus the scars on the breast are more extensive.
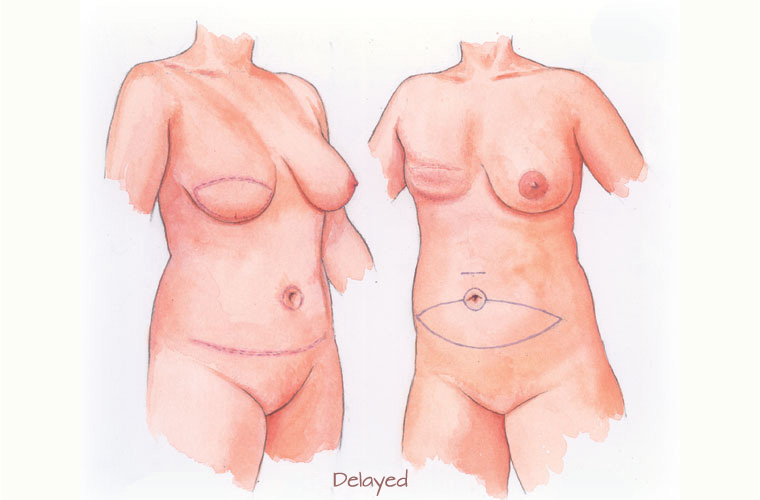
This diagram illustrates how in a delayed reconstructions more skin is required, due to the contracture of the remaining breast skin after a mastectomy as it contracts down to the chest wall. Therefore, more skin is required producing a larger skin paddle on the new breast.
Other Procedures
Please go through the information below in your own time to help your understanding of the options available.